
Abstract
Liposarcoma is a common malignant soft tissue tumor accounting for 10 per cent to 16 per cent of all sarcomas. We describe a case of 59-year-old patient presenting with a large, immobile, recurrent mass in the right mid-thigh with a different type of Liposarcoma. We have studied the case thoroughly including: X-Ray, Echo, CT, MRI, Bone Scan and Biopsy. We have planned for a radical resection of the large mass in this case, taking into consideration, the patient’s refusal of amputation. After the surgery, we put the postoperative plan including adjuvant therapy to reduce the recurrence rate of the tumor.
Introduction
Liposarcoma is a common malignant soft tissue tumor accounting for 10 per cent to 16 per cent of all sarcomas. It typically affects elderly between the fifth and seventh decade of life and usually develops in the extremities or retroperitoneum [1]. The World Health Organization (WHO) classifies liposarcomas to [3]: (1) well differentiated, (2) dedifferentiated; (3) myxoid; (4) pleomorphic and (5) Liposarcoma, not otherwise specified.
The respectability of the tumor and the histopathology are the most important prognostic predictors for treatment, according to that a complete excision of the tumor reduces the local recurrence rate [2]. Here we present a case of a large thigh liposarcoma, the involvement of sciatic nerve, the successful of radical resection of the mass and the histological type of recurrence represents the particularity of this case.
Case presentation
A 59-year-old male patient who was previously healthy complained of an increased enlargement in the posteromedial aspect of the right mid-thigh four years ago. The previous surgical history of the patient revealed excision of a well-differentiated liposarcoma nine months ago at the same locus. He came to our university hospital in Damascus, Syria (Albairouni University Hospital) with a complaint of a recurrent mass in his right thigh increasing in size within the last nine months immediately after the previous surgery. On admission, the examination revealed a (35x20x18) centimeter (cm) high consistency mass, immobile on the posteromedial aspect of the entire right thigh and a scar from the previous surgery (Figure 1). The clinical examination and laboratories were otherwise normal. On the plain X-ray there was an obvious enlargement of the soft tissue without ossification or calcification at the level of the mass. (Figure 2).

(Figure 1) The mass on the posteromedial aspect on the thigh.

(Figure 2) X-ray of the mass reveals an enlargement of the soft tissue without ossification or calcification.
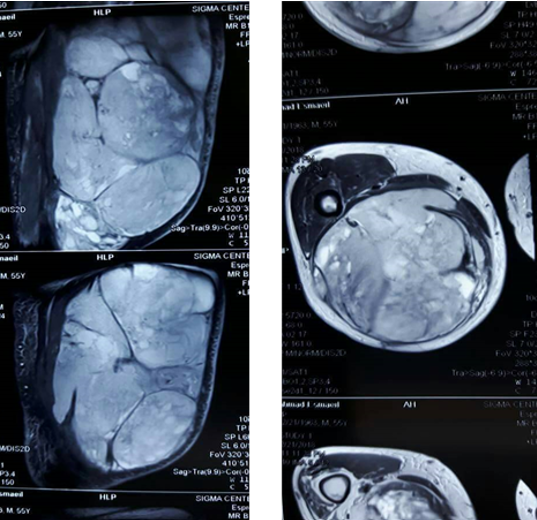
The ultrasound study showed an inconsistent without obvious boundaries mass with peripheral vascularization in the right thigh with an edema in the subcutaneous tissue and a free fluid in the presence of a large mass with areas of necrosis. The mass measured (35x20x18) cm and was located in the posteromedial aspect of the thigh extending from the lower border of the pelvis to the level of fatty lobules. Magnetic Resonance Imaging (MRI) of the right thigh revealed the popliteal fossa which invaded the adjacent soft tissues and had a high signal on T1 weighted and STIR images (Figure 3).
(Figure 3) MRI of the mass revealed a large mass invading the adjacent soft tissue.
The femur was normal with no obvious invasion by the mass. The femoral neurovascular bundle was not affected whereas the sciatic nerve was included in the mass (Figure 3). A Whole-body Computed Tomography (CT) scan revealed no metastases. A bone scan showed an area of irregular increased radioisotope uptake in the middle of right thigh. An excisional biopsy was scheduled and the histopathology demonstrated high grade sarcoma with massive necrosis 60% and the differential diagnosis was: Liposarcoma, Malignant Fibrous Histiocytoma (MFH). The decision was made to resect the mass radically with the possibility of amputation. According to patient’s preference we perform a limb salvage surgery with beforehand knowledge of the occurrence of foot drop. We chose a posterior approach of the thigh, then we dissected it from the muscles and neurovascular bundle and resected it. The sciatic nerve was identified at the greater sciatic foramen, and it was included within the mass. We performed a wide resection of the muscles in the posterior compartment of the thigh including parts of semitendinosus, semimembranosus and Biceps Femoris muscles. The sciatic nerve was resected from the greater foramen to the popliteal fossa. The resected mass weighed about 25 kilograms (Figure 4).
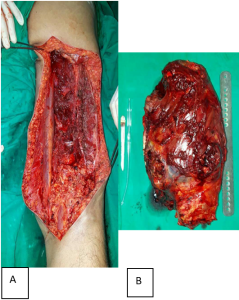
(Figure 4) A. The surgical approach on the posterior aspect of the femur. B. The resected mass.
The histopathology studies revealed the diagnosis of Myxoid Liposarcoma with free resection borders (Figure 5). The patient was put on an ankle foot orthosis (AFO) and multimodality treatment is scheduled to be applied for its beneficial impact [8]. The patient also after receiving multimodality treatment will undergo tendons transfer or ankle arthrodesis for the foot drop.
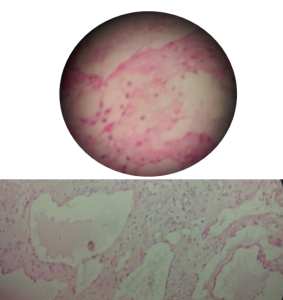
(Figure 5) Histopathology of the mass showed Myxoid Liposarcoma.
Discussion
Liposarcomas are the most frequent soft-tissue sarcomas. The WHO classifies these tumors to five main histological types: well-differentiated, dedifferentiated, myxoid, pleomorphic and Liposarcoma, not otherwise specified. Well-differentiated liposarcoma considered locally aggressive with no potential for metastasis [3]. Liposarcoma types range from non-metastatic tumors (well-differentiated liposarcoma) to tumors with high metastatic potential (pleomorphic liposarcoma) [4]. Myxoid liposarcoma is particularly radiosensitive thus neoadjuvant radiation protocols may be very effective. [5]
Local recurrence is common, occurring in two thirds of all liposarcoma patients. Metastases are also common, occurring in 50% of patients [6]. Most recurrences of soft-tissue sarcomas of the extremities occur in the first two years after primary treatment [7].
In this case the previous diagnosis was well-differentiated liposarcoma and the present diagnosis revealed a myxoid liposarcoma which gave rise to many queries including the recurrence with complete new tumor or transforming from a residual previous tumor or the present tumor is just a subtype of dedifferentiated liposarcoma etc.
Conclusions
Liposarcoma is one of the most common forms of soft tissue sarcoma and has several subtypes. These tumors can reach to large sizes which makes complete surgical resection with free surgical borders a real challenge. Metastases are another important issue to take into consideration when dealing with large tumors. Many authors correlate metastases to the tumor size, but in our case, there were not any metastases although the tumor’s large size. Multimodality treatment after surgery has a valuable benefit.
References:
1- Conesa X, Seijas R, Ares O, Huguet P, Perez M. Multicentric liposarcoma. Acta Orthop Belg. 2011;77: 9-14
2- Henze J, Bauer S. Liposarcomas. Hematol Oncol Clin North Am 2013;27(5):939e55.
3- Fletcher CDM, Bridge JA, Hogendoorn PCW, Mertens F, editors. WHO Classification of Tumours of Soft Tissue and Bone. Pathology and Genetics of Tumours of Soft Tissue and Bone. 4th ed. Lyon: IARC Press, 2013.
4- Murphey MD, Arcara LK, FanburgSmith J: From the archives of the
AFIP: Imaging of musculoskeletal
liposarcoma with radiologicpathologic correlation. Radiographics 2005; 25: 1371-1395.
5- Prestwich RJ, Taylor RE, Grimer R: Metastatic myxoid liposarcoma: aggressive multimodality management. Clin Onc 2005,; 17:130-134.
6- Peterson JJ, Kransdorf MJ, Bancroft LW, O’Connor MI. Malignant fatty tumors: classification, clinical course, imaging appearance and treatment. Skeletal Radiol. 2003; 32:493-503.
7- Whooley BP, Gibbs JF, Mooney MM, McGrath BE, Kraybill WG. Primary extremity sarcoma: what is the follow-up? Ann Surg Oncol. 2000;7(1):9-14.
8- Dalal KM, Antonescu CR, Singer S. Diagnosis and management of lipomatous tumors. J Surg Oncol. 2008 Mar 15. 97(4):298-313.
Authors:
Ali Mahmoud, Ph.D; Muhammad Rafat Meda, MD; Muhammed Fayez Aboujaib, MD.
Department of Orthopaedic Surgery, Damascus University, Damascus, Syria.
Corresponding author: Muhammad Rafat Meda; Rafat.meda@gmail.com; +963949119583.
Institution of all authors: Albairouni University Hospital, Damascus, Syria.
E-mail: bairouni@tarassul.sy ; Telephone: 00963-11-2130165; Fax: 00963-11-2130171
Images submitted by the authors
To reference this article, please use:
Mahmoud A, Meda MR, Aboujaib MF, Limb Salvage Surgery: A Case Report of Large Thigh Liposarcoma, Orthopaedic Product News, 2020 September (https://bit.ly/2E8tutC)
